| Overview |

| Aboriginal children and families are significantly over-represented in the child protection system. This is a direct result of continuing harm caused by past acts, policies, and legislation, including the Aborigines Act 1905 (WA), with the purpose of 'protection, control, and segregation' of Aboriginal people.
The Department of Communities (Department) acknowledges the historical legacy of separation of children from families and communities, the suppression of Aboriginal values such as culture and language, and the ensuing cultural dislocation, intergenerational trauma, grief, and loss.
The Department actively acknowledges and promotes the fundamental role of family, community and the right to participation and self-determination having the autonomy in the protection and care of Aboriginal children.
|
A Child Safety Investigation (CSI) is undertaken by authorised officers from the Department of Communities (the Department). A CSI is the outcome of an Interaction or Initial Inquiry and is recorded in Assist. Progression to a CSI must be approved by a team leader. A CSI must be completed within 30 calendar days and is conducted under the provisions of Section 31 and 32 of the
Children and Community Services Act 2004 (the Act). Refer to the
Child Safety Investigation Flowchart for more context (in related resources) |
| Rules |
Three practice requirements must be determined as part of a CSI:
Whether or not the child has experienced harm or is likely to experience harm as a result of the abuse
The parent's capacity to protect the child from harm, and
Whether the child is in need of protection.
These determinations must be made in the context of s.28 of the Act, which identifies when a child is in need of protection.

| You must consider the context of the family and household members, including any siblings or other children affected, when conducting a CSI.
This includes any other child in a care arrangement where concerns have been raised about a carer and a carer investigation is to occur.
|
For investigations relating to children in the CEO's care please refer to entries 2.1.4 – 2.1.7 Responding to Concerns for Children in the CEO's Care or 2.1.8 Responding to Concerns about Employees.
|
| Process Maps |
- Referral process concerning young people, or families at risk of radicalisation to violent extremism
- Child Safety Investigation Flowchart
|
Information and Instructions- Timeline of a Child Safety Investigation
- Culturally responsive practice
- The relationship between abuse and harm
- Referrals requiring a specific response
- Investigative actions
- Using Signs of Safety
- Interviewing the child
- Working with WA Police Force
- Assessing harm
- Assessing a parent's capacity to protect
- Writing the Outcome Report
- Approvals
- Actions following approval
Timeline of a Child Safety InvestigationYou
must use the
Interaction Tool in related resources to determine whether or not to proceed with a CSI.
When you proceed with a CSI at the conclusion of an Interaction or Initial Inquiry, a priority level must be selected that determines the timeline for commencing the investigation.
Priority 1 =
must be commenced within 24 hours.
Priority 2 =
must be commenced within 2-5 calendar days.
|
| You
must: 1. Consult with your team leader when making a decision about the appropriate priority response. 2. Select an abuse type correlating to
s.28 of the Act to progress to a CSI; this is the grounds under which the investigation is taking place. |
A decision regarding the parent's capacity to protect and the decision date can be recorded at any time during the 30 calendar days.
You are not required to send the CSI for approval immediately after recording these decisions. For example, where you know the likely outcome and are waiting to complete the final right of reply meeting, you can record in Assist a value for the parent's capacity to protect and the CSI decision date. You can then save the CSI, which will remain open, and complete the remaining items when you send the CSI for approval.
Selecting a priority level

| Whichever priority you record when intaking an Initial Inquiry will remain in place if you later progress to a CSI. |
The following tables detail considerations for Priority 1 and Priority 2 responses.
Age of the child
Priority 1 considerations |
Priority 2 considerations | Children aged 0-5 years are especially vulnerable but older children are also vulnerable when severe injury or threat is present OR
Infants and children (under 3 years of age) are determined to be at increased likelihood of harm as the result of risk factors (high risk infants) | Children aged 0-5 years, with younger or developmentally immature children being especially vulnerable
|
Functioning and developmental stage of child
Priority 1 considerations |
Priority 2 considerations | Child is significantly below chronological age, has severe physical, developmental, mental disability or illness. | These vary from children whose development is below chronological age or have minor physical or mental developmental disability or illnesses requiring some adult assistance to children where functioning is age appropriate and there is no physical or mental developmental disability or illness. |
Severity of injury
Priority 1 considerations |
Priority 2 considerations | Life threatening injury requiring immediate medical attention, sexual penetration or injury, torture, chronic long term harm | Ranges from physical harm and sexual harm which may require medical documentation or monitoring to chronic/persistent neglect or emotional abuse which is not life threatening |
Location of injury
Priority 1 considerations |
Priority 2 considerations | | Head, face, genitals, internal organs | Injuries on the torso and soft tissue areas may be more serious than injuries located on bony body parts, knees, elbows and buttocks |
Recency of harm
Priority 1 considerations |
Priority 2 considerations | | Same day as report, currently occurring | Ranges from events which occurred within one week of the referral to events which happened longer than one week ago |
Previous incidents
Priority 1 considerations |
Priority 2 considerations | | Previous substantiated harm or likelihood of harm involving the child or siblings, or a person involved has been identified as Assessed as Causing Significant Harm (ASH) or Actual Harm Continuing Risk (AHCR) | Previous substantiated harm or likelihood of harm involving the child or siblings, or a person involved has been identified as Assessed as Causing Significant Harm (ASH) or Actual Harm Continuing Risk (AHCR) |
Likelihood of recurrence
Priority 1 considerations |
Priority 2 considerations | | Significant likelihood that further harm or issues associated with a concern for a child will re-occur | Quicker response required when there is indication that harm may re-occur within the 2-5 day timeframe |
Chronicity or persistence
Priority 1 considerations |
Priority 2 considerations | Considered together with the severity of harm and includes events where a single incident is associated with severe harm likely to have long term effects; also persistent, chronic, ongoing events which will also have long term effects (for example, chronic neglect of babies which is life threatening) | Considered together with indications of severity of injury and may include allegations where events have been spasmodic or once off but where injury has been significant, to concerns where injury has not been significant or there has been no injury |
Intent of person we are worried about
Priority 1 considerations |
Priority 2 considerations | | Deliberate intent to cause harm | Intent cannot be ascertained or is not present; self-control is not significantly impaired through psychiatric illness, substance abuse or developmental disability, or other adults provide for safety |
Access to child by person we are worried about
Priority 1 considerations |
Priority 2 considerations | Easy, ongoing access to child by a person we are worried about | May include situations where access to a child by the person we are worried about or a person previously responsible for violence within the family is controlled by a family member or by legal provisions such as restraining orders to situations where there is no access to the child or non-abusing/non-violent caregiver |
Current location of child(ren)
Priority 1 considerations |
Priority 2 considerations | Child currently alone or in sole care of the person we are worried about | Child in the care of a caregiver who is protective or is in a place of safety where access by person believed responsible or of concern can be denied |
Protectiveness of caregiver
Priority 1 considerations |
Priority 1 considerations | | No caregiver available, willing or able to care for and protect child | Previous incidents have not been life threatening or severe, or have not been confirmed (there may have been no previous incident). This may vary from situations where there are doubts about a non-abusing caregiver's ability to protect, or access to support which enables protection of the child, to situations where the caregiver is clearly willing and able to protect the child (or ensure safety in family violence situations) |
Capacity of caregiver to provide care for the child
Priority 1 considerations |
Priority 2 considerations | | Caregiver's parenting capacity significantly affected by psychiatric illness, alcohol or drugs, or developmental disability | Previous assessments regarding parenting capacity found there were chronic low-level concerns which were improved with safety planning AND no significant mental health issues, AOD or developmental disability; OR no previous concerns but family is currently undergoing a crisis where parenting capacity has been affected AND no significant mental health issues, AOD or developmental disability |
Precipitating events
Priority 1 considerations |
Priority 2 considerations | | Ongoing, likely to re-occur frequently | This may vary from events which have been frequent or which are predictable to events that are unlikely to re-occur |
Stress factors present
Priority 1 considerations |
Priority 2 considerations | Family stress factors and distress of person we are worried about or about whom concern is high | May include situations where family stress, distress of person believed responsible for harm or about whom there is concern is present but not severe |
Information from other agencies
Priority 1 considerations |
Priority 2 considerations | Family known to other agency; agency has significant concern about imminent risk of harm to child | Information obtained from other agencies will provide information about indicators as well as perception of risk and safety issues |
Protective behaviour of caller
Priority 1 considerations |
Priority 2 considerations | Caller unable or unwilling to provide short term protection of the child | The willingness and ability of the caller to provide immediate or longer term protection or support will impact on response type and time |
Commencing a CSI in Assist
Navigate to the CSI from the 360 Degree View screen. You
must have an approved Case Plan to do this.
- Use the Calendar icon to insert date and time. Select navigate to CSI to open the CSI page and select the Save button in the top left corner.
- The CSI will progress from 'initiated' to 'commenced'.
- Once the CSI is active, record the parents' capacity to protect.
Entering parent's capacity to protect
- Navigate to the CSI from the 360 Degree View. You
must have commenced a CSI for the screen to be active.
- Scroll to the bottom of the screen to the 'Parents Capacity to Protect' section. It is located between 'Involvement' and 'S33 Details'. Make sure you are ready to record your decision about the parent's capacity to protect their child, as once you enter values in this section, and saved the page, this section cannot be edited further.
- Record a response under 'Capacity' of either 'Yes', 'Unknown', or 'No'. Only a response of 'Yes will allow you to select 'Complete Assessment' under the Action section.
- Record the date in the appropriate section and record an 'Action' from the drop down menu. The time will populate automatically.
- Save the CSI screen.
Entering Decision Date
- Navigate to the CSI from the 360 Degree View. You
must have recorded the Parents Capacity to Protect in order to record the Decision Date.
- Scroll to the bottom of the page to the Decision Details section. It is located between 's33 Details' and 'Parties Notified of Decision of Child Safety Investigation'.
- Complete all the available sections under Decision Details, especially the date boxes, and save the CSI screen. The items under Decision Details will remain editable until the CSI is sent for approval.
Receiving new concerns to an open investigation
If you are already undertaking an investigation in relation to a child and you receive new concerns for that child, in
consultation with a team leader, you should decide if a new interaction is recorded or if the new concern is addressed as part of the current open investigation.
If the new concerns relate to child sexual abuse and you form a belief, on reasonable grounds, that sexual abuse to a child has occurred, or is occurring, then you
must refer to entry 2.2. Mandatory Reports of Child Sexual Abuse.
If… |
Then… | The new referral contains information regarding the same abuse type as the current open investigation
| The referral can be recorded as additional information and addressed as part of the current investigation | | The new referral contains information significantly different from the current open investigation or in relation to a different relative | The referral should be recorded as a new interaction and an intake |
The decision about recording a new referral as additional information or as a new investigation is made in consultation with the relevant team leader, yours, and/or the team leader responsible for the current investigation.
After hours investigations When the Crisis Care Unit (CCU) receives information out of hours and assesses a case as warranting an investigation, the CCU commences the investigation process. If the CCU does not complete the investigation, they refer the investigation to the responsible district office as soon as possible. TopCulturally responsive practiceWhen you identify a child or family as Aboriginal and/or culturally and linguistically diverse (CaLD), you must consult with the Aboriginal practice leader (APL) or the Cultural Diversity team in the Specialist Child Protection Unit (email: SCPU_Cultural_Diversity@communities.wa.gov.au) as soon as possible to gather information to assist in engaging with the parents.
You must document the consultation either via a case note,
using Form 456 - Request for Consultation with the APL, or using the Assist function. For CaLD consults, the Cultural Diversity officer will summarise the main recommendations and the discussion held in a formalised email which is to be placed on the Case File in Objective. This consultation is to assist you to develop an effective plan for your investigation that takes into consideration cultural issues.
Working with Aboriginal and Torres Strait Islander families
It is important to open meetings with an Acknowledgement of Country as a way of paying respect to the Aboriginal and Torres Strait Islander people who are the custodians of the land where the meeting is taking place. An Acknowledgement of Country from our staff is part of the empowerment strategy to encourage self-determination and supports keeping culture at the heart and securing a strong foundation at the start of our work with families. We must remember also that some of the families we work with are off Country. Refer to the Aboriginal Cultural Hub for further information. You should review the resource Stronger Safer Together which is a reflective practice resource and toolkit for services providing intensive and targeted support for Aboriginal and Torres Strait Islander families, developed by the Secretariat of National Aboriginal and Islander Child Care (SNAICC). When working with Aboriginal families, you should, in consultation with the APL, use the Tindale Map to identify (where possible) each parents' cultural group and languages spoken. The Tindale Map of Indigenous Australia is developed by the Australian Institute of Aboriginal and Torres Strait Islander Studies (AIATSIS). Where families have experienced intergenerational trauma and multiple contacts with child protection directly or indirectly, it is important to acknowledge the past and actively listen to the family to begin to develop a working relationship, and for the conversations to begin. This might include statements such as:

|
"I know it's hard to talk to me / you might not want to talk to me, but this is really important…"
I know some of your family have been in care and have had a really rough time, I don't blame you for not wanting to talk to me…" |
|
Working with Culturally and Linguistically Diverse families When working with CaLD families, you should, identify, where possible, each parent's country of origin, cultural group and language spoken. The
Cultural Prompt List can assist with gathering this information. Where parents may have a background of trauma, you should approach them with empathy and recognise their difficult experiences. If the parents choose to share this experience, you should listen with genuine interest and allow the parents to tell their story. When families have never had contact with the child protection system or feel anxious about the Department contacting them, it is important to reassure them, for example:
|
| "It is possible you have never been through this before… I know this may feel intrusive, make you feel embarrassed and/or worry you that other community or close family members/friends may hear, or you may feel that I am here to take your child/ren away or break up your family, but…"
|
|
Parents from CaLD) backgrounds may have experienced trauma, sexual assault, violence, loss and grief in their country of origin and/or refugee camps, resulting in post-traumatic stress, anxiety, depression and/or other mental health difficulties. The effect of this trauma can inhibit some parents from bonding with and caring effectively for an infant and make it more difficult for them to engage in support. Where trauma is identified as impacting on parents, workers should contact the cultural diversity team to explore culturally appropriate supports and services via SCPU_Cultural_Diversity@communities.wa.gov.au.
Pregnant women and new mothers from CaLD backgrounds can be at heightened risk of anxiety, depression, post-natal depression, social isolation and family and domestic violence. Protective factors and strengths for CaLD women and families can include: - having the ability to move around the community freely (others not controlling movements);
- having friendships outside of the home;
- engaging with neighbours, services and others in the community;
- having access to transport when required (including access to public transport); and
- having their own phone and access to finances.
Where parents may have a background of trauma, you should approach them with empathy and recognise their difficult experiences. If the parents choose to share this experience, you should listen with genuine interest and allows the parents to tell their story. Harmful cultural practices can include female genital cutting and mutilation, arranged or forced and early marriages, honour killings or attempted honour killings, and the payment of dowries. These practices can also involve family and domestic violence. You should have separate conversations with parents to screen for harmful cultural practices and family and domestic violence. When gathering information about cultural (and where relevant, religious) practices (and harmful cultural practices), use a 'naïve enquirer' approach to 'fact check', for example: |
| |
"If someone was worried about your child in your home country, what would happen?... Who would you talk to about what was happening?
Who would give you the most help?"
"In your home country, if a Mum was feeling very, very sad after giving birth, what would happen?"
"Would someone in your situation (e.g. arranged marriage) be able to go out on her own / catch public transport / go to the shops?" |
|
Where required, you should refer parents to appropriate trauma informed support and mental health services: When working with Aboriginal and CaLD families, you should consult with specialist staff (such as the APL and/or the Cultural Diversity officer of the Cultural Diversity team in the Specialist Child Protection Unit - SCPU_Cultural_Diversity@communities.wa.gov.au and/or access resources and information specific to the family's cultural group and religion (if relevant) to plan for how best to engage the parents and deliver culturally responsive practice.
Use a 'naïve enquirer' approach with parents to gather information about their cultural practices, religious beliefs, family 'norms' and parenting practices, including screening for family and domestic violence. Consider the family's experience of trauma, intergenerational trauma and possible past contact with child protection systems.
Where there are cultural considerations which may prevent both parents from engaging with the Department you should seek guidance from the:
- APL and/or
- the Cultural Diversity officer in the Cultural Diversity Team in SCPU and
- other staff and resources to plan for how to best to engage both of the parents.
You can also 'fact check' with parents and families what the cultural expectations are for them according to gender: |
|
"What kind of role do men take in your family?"
"I would like to talk to Dad but I know it might not be culturally appropriate for him to speak with me. Who is the best person to talk to Dad?" |
|
|
| Cultural safety occurs when a person is not in fear of racism or discrimination. They feel spiritually, socially, emotionally and physically safe to be themselves. You can 'set the scene' for cultural safety by approaching parents in a respectful and non-judgemental way, not 'speaking down' to the parents and showing a genuine interest in what they have to say. |
For more information on culturally responsive practice, refer to SNAICC's
Implementation of the Aboriginal and Torres Strait Islander Child Placement Principle resource, the Cultural Support Panning Creating Cultural Safety, and the CALD Hub.
The relationship between abuse and harmThe Department's role in a CSI is to investigate abuse and determine whether the child has suffered physical, emotional or psychological harm to the level that it has had a
detrimental effect of a
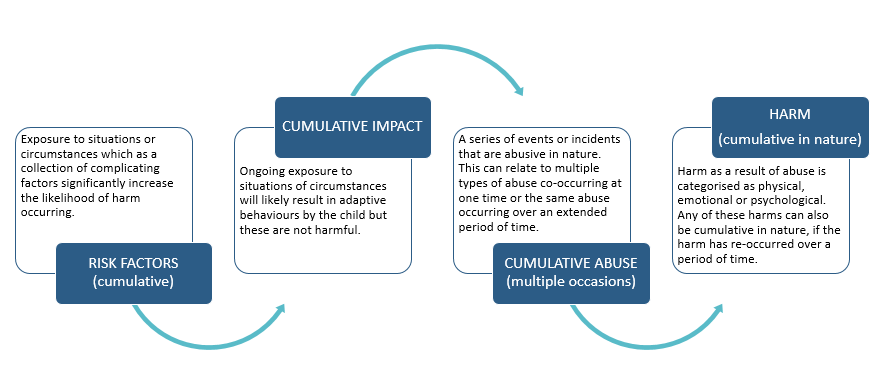
significant in nature as a result of abuse and/or neglect as identified in s.28 of the Act. Where 'abuse' is an action or inaction against a child, 'harm' refers to the detrimental effect or impact of that action or inaction on the child. Harm is defined in s.3 of the Act as harm to the child's physical, emotional or psychological development. Harm can be the result of a single act, omission or circumstance, or a series or combination of acts, omissions or circumstances (previously referred to as cumulative harm).

| You must develop a harm statement whenever harm is substantiated. |
Definitions of abuse Abuse is an act or failure to act towards or on behalf of a child that may result in harm. Abuse can occur on one or multiple occasions; we have previously referred to these concepts as an "omission of care" or "cumulative harm". It is possible to have cumulative abuse (multiple events over time) that results in harm that is cumulative in nature (the impact of the events has been cumulative). The abuse types and grounds for when a child is in need of protection are identified in
s.28 of the Act.
Abuse type and section in the Act
Physical abuse s.28(2)(c)(i)i) |
Physical abuse occurs when a child has suffered severe and/or persistent ill-treatment through behaviours such as beating, shaking, inappropriate administration of alcohol, drugs and medicines, attempted suffocation, excessive discipline, excessive physical punishment, scalding, shoving, hitting, slapping, kicking, biting, burning, strangling, poisoning, female genital mutilation.
Common measures to determine if physical punishment of a child is reasonable could include the age and size of the child, the method of punishment, the child’s capacity for reasoning and the harm caused to the child.
Section 257 Criminal Code 1913 states:
It is lawful for a parent or a person in place of a parent, or for a schoolmaster, to use, by way of correction, towards a child or pupil under his care, such force as is reasonable under the circumstances.
Physical Abuse Policy |
Sexual abuse s.28(2)(c)(ii) |
‘Sexual abuse’, in relation to a child, includes sexual behaviour in circumstances where: - the child is the subject of bribery, coercion, a threat, exploitation or violence; or
- the child has less power than another person involved in the behaviour; or
- there is a significant disparity in the developmental function or maturity of the child and another person involved in the behaviour.
Sexual abuse occurs when a child has been exposed or subjected to sexual behaviours that are exploitative and/or inappropriate to his/her age and development level. Examples of this include sexual penetration, inappropriate touching, exposure to sexual acts or pornographic materials and using the internet for grooming and soliciting children for sexual exploitation. Sexual activities between young people are not considered as sexual abuse unless: - it is non-consensual or there are concerns about the young person’s capacity to give consent
- there are factors such as bribery, coercion, threats, exploitation or violence
- the child has less power than the other person, or
- there is significant disparity in the developmental function or maturity.
Child sexual abuse can be broadly categorised as ‘intra-familial’ or ‘extra-familial’ child sexual abuse.
Intra-familial child sexual abuse is perpetrated by a person who is a relative of the child or has a kinship relationship with the child. This applies to any child under 18 years of age. The term 'relative' in relation to a child is defined in s.3 of the Act as: (a) the child's:
- parent, grandparent or other ancestor
- step-parent
- sibling
- uncle or aunt
- cousin
- spouse or de facto partner
whether the relationship is established by, or traced through, consanguinity, marriage, a de facto relationship, a written law or a natural relationship. (b) in the case of an Aboriginal child, a person regarded under the customary law or tradition of the child's community as the equivalent of a person mentioned in paragraph (a) above, and (c) in the case of a Torres Strait Islander child, a person regarded under the customary law or tradition of the Torres Strait Islands as the equivalent of a person mentioned in paragraph (a) above.
Extra-familial child sexual abuse perpetrated by a person who is not a relative of the child or by a person outside the child or young person's kinship system. The Department does not generally investigate allegations of extra-familial sexual abuse, unless there are concerns about the parent's capacity to protect the child following the application of the
Interaction Tool.
Child Sexual Abuse Policy |
| Staff must consult with appropriate Aboriginal staff in their districts or with the Senior Advisor, Aboriginal Services or the Senior Advisor, Cultural Diversity, with regards to kinship relationships |
Emotional abuse (including family and domestic violence and psychological)
s.28(2)(c)(iii) |
Emotional abuse is the sustained, repetitive, inappropriate, ill-treatment of a child or young person through behaviours including threatening, belittling, teasing, humiliating, bullying, confusing, ignoring and inappropriate encouragement.
The term ‘emotional abuse’ includes psychological abuse (the sustained, repetitive, inappropriate, ill-treatment of a child or young person through behaviours including threatening, isolating, neglecting, discrediting, misleading, disregarding, ignoring and inappropriate encouragement) and exposure to family and domestic violence, which causes serious emotional, psychological and physical harm to children, as well as placing them at increased likelihood of abuse and neglect. Emotional Abuse - Family and Domestic Violence Policy |
Neglect s.28(2)(c)(v) |
Neglect is when a child is not provided with adequate food or shelter, effective medical, therapeutic or remedial treatment, and/or care, nurturing or supervision to a severe and/or persistent extent where the health or development of the child is significantly impaired or placed at serious risk.
It includes failure by a child's parents to provide, arrange or allow the provision for adequate care for the child or effective medical, therapeutic or remedial treatment for the child.
Neglect Policy |
Other legislative grounds for intake |
Abandonment- Section 28(2)(a)(i) and (ii) - the child has been abandoned by their parents and, after reasonable enquiries the parents cannot be found; and no suitable adult member of the child's family or other suitable adult can be found who is willing and able to care for the child OR Section
28 (2)(aa) (i) and (ii)) – on the parent or parents being found there is no parent who is willing and able to care for the child and no suitable adult member of the child's family or other suitable adult can be found who is willing and able to care for the child. Dead or incapacitated - Section 28(2)(b) - the child's parents are dead or incapacitated and no suitable adult member of the child's family or other suitable adult can be found who is willing and able to care for the child. Unable or unwilling to provide adequate care - Section 28(2)(d)(i) and (ii) - the child has suffered or is likely to suffer harm as a result of the child's parents being unable or unwilling to provide, or arrange the provision of, adequate care for the child OR the child's parents being unable or unwilling to provide, or arrange the provision of, effective medical, therapeutic, or other remedial treatment for the child.
|
Types of harm Harm is the impact of abuse; it is the detrimental effect on the child and significant in nature. Harm is categorised in s.3 of the Act as the impact on a child's physical, emotional or psychological development. A child may suffer physical harm, emotional harm or psychological harm as a result of abuse. It is possible to have cumulative abuse that results in harm that is cumulative in nature. Physical harm – Evidence of impact on the child's physical body, can be internal or external in nature. Emotional harm – Evidence that the abuse or neglect has affected how the child feels, for example, how the child feels about themselves and the world around them. Psychological harm – Evidence that the abuse or neglect has impaired or impeded the mental life or mental development of the child. The mental life includes things like intelligence, memory, recognition, perception, attention, imagination and moral development.
Abuse types (grounds for investigation) and evidence of harm for physical abuse, sexual abuse, emotional abuse (including emotional abuse FDV and psychological abuse) and neglect, and how they can impact on the child (including but not limited to):
Evidence of harm/impact on child | Physical harm: - Bruising
- Fractures
- Internal injuries
- Burns
- Bites
- Injury as a result of penetration
- Injury as a result of FDV
- Illness and/or infection
- Malnutrition and/or dehydration
- Disease (as a result of neglect)
- Death as a result of co-sleeping
- Failure to thrive (as a result of neglect)
- Female genital cutting and/or mutilation
Emotional harm: - Sadness and/or anger
- Poor self-esteem
- Fear and/or anxiety
- Communication and/or relationship difficulties
- Drug and/or alcohol misuse
- Antisocial and/or criminal behaviour
- High levels of aggression
- Emotional regulation difficulties
- Dissociation
- Suicidality
- Somatization (physical symptoms from distress)
- Poor interpersonal skills and relationship dysfunction
Psychological harm: - Sadness and/or anger
- Poor self-esteem
- Fear and/or anxiety
- Communication and/or relationship difficulties
- Drug and/or alcohol misuse
- Antisocial and/or criminal behaviour
- High levels of aggression
- Emotional regulation difficulties
- Dissociation
- Suicidality
- Somatization (physical symptoms from distress)
- Poor interpersonal skills and relationship dysfunction.
|
Abandonment s.28(2)(a)(i)(ii) and s.28(2)(aa) (i)(ii) the child has been abandoned by their parents and, after reasonable enquiries the parents cannot be found; and no suitable adult member of the child's family or other suitable adult can be found who is willing and able to care for the child OR on the parent or parents being found there is no parent who is willing and able to care for the child and no suitable adult member of the child's family or other suitable adult can be found who is willing and able to care for the child.
Dead or incapacitated s.28(2)(b) Child's parents are dead or incapacitated and no suitable adult relative or other suitable adult can be found who is willing to care for the child. | The Act does not allow for the consideration of harm in relation to these sections, therefore the recorded outcome is 'intervention action'.
Under s.28(2)(a)(i)(ii) and s.28(2)(aa)(i)(ii) of the Act, abandonment can only apply when we cannot locate a parent or suitable adult family member OR when on the parent or parents being found there is no parent who is willing and able to care for the child and no suitable adult member of the child's family or other suitable adult can be found who is willing and able to care for the child.
Under both these sections, although there are grounds for the child to enter care, these are not a direct result of parent’s actions, therefore they cannot be held accountable for harm. The parents have acted out of incapacity or inability, rather than with intention to harm their child.
|
Unable or unwilling to provide adequate care s.28(2)(d)(i)(ii)
The child has suffered or is likely to suffer harm as a result of his or her parents being unable or unwilling to provide, or to arrange for the provision of adequate care for the child
OR to provide, or arrange for the provision of effective medical, therapeutic, or other remedical treatment for the child. | This section allows us to make a determination that the child has or will suffer harm regardless of the parent's inability to provide or arrange care. Physical harm:
- Bruising
- Fractures
- Internal injuries
- Burns
- Bites
- Injury as a result of penetration
- Injury as a result of FDV
- Illness and/or infection
- Malnutrition and/or dehydration
- Disease (as a result of neglect)
- Death as a result of co-sleeping
- Failure to thrive (as a result of neglect)
- Female genital cutting and/or mutilation
Emotional harm: - Sadness and/or anger
- Poor self-esteem
- Fear and/or anxiety
- Communication and/or relationship difficulties
- Drug and/or alcohol misuse
- Antisocial and/or criminal behaviour
- High levels of aggression
- Emotional regulation difficulties
- Dissociation
- Suicidality
- Somatization (physical symptoms from distress)
- Poor interpersonal skills and relationship dysfunction
Psychological harm: - Sadness and/or anger
- Poor self-esteem
- Fear and/or anxiety
- Communication and/or relationship difficulties
- Drug and/or alcohol misuse
- Antisocial and/or criminal behaviour
- High levels of aggression
- Emotional regulation difficulties
- Dissociation
- Suicidality
- Somatization (physical symptoms from distress)
- Poor interpersonal skills and relationship dysfunction.
|
For
further information on the how abuse and different harm types are recorded on Assist
then please see “Investigation of harm – Abuse & Intake Types,
Status and Outcome Options Flowchart” in related resources. Referrals requiring a specific responseThere may be contextual circumstances present in a referral which dictate a specific response from the Department. Those circumstances and information about how to respond are detailed below. If you are unsure whether a referral requires a specific response, consult with a team leader.
|
| Where you are conducting a CSI for a child in the CEO's care, you must consult and coordinate any interviews with the child and carers with the Duty of Care Team (DOCT). DOCT has the responsibility to interview carers when a carer investigation occurs. This includes instances where the carers being investigated have biological children. If two separate Intakes are completed (one for the children in the CEO's care and another for biological children), workers completing the CSI's should work collaboratively and in consultation with DOCT.
|
For information and instructions refer to the resource Referrals requiring a specific response (also in related resources). This resource includes practice guidance on the following: Mandatory Reports of child sexual abuse
Medical child abuse
Undertaking a CSI with parents who are under the age of 18 Children younger than 5 years of age
Recommendations on restricted child/prisoner visits Foetal Alcohol Spectrum Disorder (FASD) Early and/or forced marriages (EFM) Family Relationship Centres and the Family Relationship Advice Line Radicalisation to violent extremism (RVE) of young people, or their parents.
Investigative actionsChild Safety Investigations are designed to address and assess the initial or immediate child protection concerns for a child. As part of a CSI, you must take actions to gather credible evidence in order to assist them in making a determination.
|
| Worker safety during client contact is a priority for workers, managers, and Communities as a whole. Worker safety must be considered before contact with children and their families. Worker safety is based on a hazard identification and risk management approach to all contact with clients. This should be undertaken before contact with clients to ensure worker safety at all times. Please see related resource
Worker Safety during client contact and home visits for guidance around considerations to keep workers safe.
|
The following actions are recommended in order to gather sufficient information to address the three practice requirements of a CSI:
Whether or not the child has experienced harm or is likely to experience harm as a result of the abuse
The parent's capacity to protect the child from harm; and
Whether the child is in need of protection.
|
The Signs of Safety Child Protection Practice Framework should be used throughout the investigation to promote engagement with parents and families. For more information go to the next section 'Using Signs of Safety'. |
|
| You are encouraged to consult with other professionals throughout the investigation process, this might include talking to: - Senior practice development officer (SPDO)
- Aboriginal practice leader (APL)
- Team leader (TL)
- Other senior workers
- Specialist Child Protection Unit (SCPU)
|
Credible Evidence The Department's standard of proof is the balance of probabilities, whereas the standard of proof for criminal matters is beyond reasonable doubt. 'Balance of probability' is defined as
somethingthat is more likely than not. We are required to gather credible evidence that will support the outcome of our investigation on the balance of probabilities. Credible evidence can include: - verbal statements
- medical evidence
- photographic evidence
- observations, including behavioural indicators
- relevant information from other agencies
- hearsay evidence that has been corroborated, and/or
- witness to the harm.
Timeline of Investigative Actions In the timeline of a CSI, there are five investigative actions that you
must undertake. They include: - Immediate safety planning.
- Notify the parents.
- All the parents the opportunity to respond.
- Sight and/or interview the child.
- Notify both parents of the likely outcome of the investigation.
These are the
minimum actions expected of you when completing a CSI. They are focused on procedural fairness and the voice of the child. You can complete these actions in the order best suited to your investigation. You
must use professional discretion and judgement to determine what other actions you might undertake as part of the investigation, in order to gather credible evidence and make a comprehensive assessment.
Whilst actions below are not requirements for every investigation, it is expected that you will undertake any other suitable actions relevant to your investigation. Other actions you take should be relevant to the type of abuse and harm you are investigating. Other suitable actions may include, but are not limited to: - using the Signs of Safety tools to engage with the parents and family
- making further contact with the original referrer
- contacting other family members
- contacting the school, general practitioner, and other services involved with the child/family to gain up to date assessments of the child/family
- contacting WA Police Force (WA Police)/WA Health under
s.23 of the Act to request relevant information
- Consider undertaking a Connect for Safety search for the family if there is information to indicate that the family may have lived in another state, or if the family has been transient, or have no history or gaps in the history with the Department. For More information, refer to
Chapter 2.2 Connect for Safety.
-
requesting information from interstate when you know the family have relocated (AAA Form 901)
- completing an initial or immediate safety plan
- making home visits to observe the child's environment
- interviewing witnesses about any alleged harm
- obtaining relevant assessments or records, e.g. health, psychological
- making referrals to services, and/or
- providing social services.
|
| Children with known disability or serious ongoing health issues are at a greater risk of experiencing abuse, including neglect. When conducting a CSI for a child with disability and/or serious health conditions, you should make a s.23 request for information to Perth Children's Hospital and other service providers as soon as practicable. Gather information about any missed appointments, note any difficulties the family are having adhering to medical plans and any upcoming appointments. This information will inform your assessment and provide important information on what additional support may benefit the child and family.
|
1. Immediate safety planning
You may need to conduct immediate safety planning at any given point in the life of an investigation (refer to chapter
2.2 Signs of Safety - child protection practice framework for guidance on safety planning, including developing harm and/or danger statements and safety goals). You need to be responsive based upon information you receive as a result of investigative actions undertaken. This might mean that there are investigations that require immediate safety planning and other investigations where it is not required. Conduct safety planning in collaboration with parents, children, families and professionals. Please refer to the steps below for guidance regarding immediate safety planning: You
must have clear danger statements and safety goals before commencing safety planning. These state our grounds for involvement and what we need to see achieved to end our involvement. Think about completing a safety scale at the commencement of safety planning - this lets everyone know how worried people are at the commencement of safety planning and can be used to review whether safety planning is required later. Use detailed questions to elicit strengths and safety. Talk to the parents, children and family about their safety networks. Be clear about your bottom lines and non-negotiables. Remember, these cannot be coercive and must operate within our legislation. Try to discuss these with a senior worker or team leader prior to planning with the family. Timeframes. An immediate safety plan may only be required for a few days while you undertake some investigative actions to determine whether longer term safety planning is actually required. Give an indication about when you are going to review the safety plan and ensure that you document a rationale if a safety plan is no longer required. Monitoring. How will you know if the safety plan is/isn't working?
|
| If you have completed an immediate safety plan early in the investigation and later assess that a longer term, formal safety planning is required, you should try to complete the investigation and progress the matter to Intensive Family Support for comprehensive safety planning to be undertaken. |
Suggested wording: |
|
"Thanks for allowing us to come and meet with you.
As part of our investigation we need to do some safety planning about what we've talked about today".
"Developing a safety plan is really critical at the moment, because it ensures that we have a shared understanding about what is happening over the next few days".
"A safety plan will reassure me that there is a clear plan in place for the children to be safe, while the adults do some actions".
"Once we've done the actions in this safety plan, I'll have more information and we can come back together to discuss whether further safety planning is required or if all our worries have been addressed" |
|
2. Notify parents The Department
must apply procedural fairness to actions taken as part of a CSI. This begins by notifying both parents, where it is safe to do so, of the investigation and the grounds for the investigation. You should consider when the parents are to be advised and by whom. The decision to delay advising or to not advise the parents of our intention to talk to, interview, examine or sight the child should be planned and the rationale documented, including consideration of the impact on the child. |
| -
Unless there is a court order directly affecting the parental rights of an individual, then both parents, regardless of caring time, have equal parental right.
- You must assume that family and domestic violence is a factor in all cases and screen out for this. As much as possible you should try to hold initial conversations with parents separately. This allows for FDV screening to occur, but also minimises the likelihood that the parents will influence each other’s recall of events.
|
You can contact parents by: - phone,
- in person,
- in a home visit, or
- by letter.
| You should use the Signs of Safety framework when engaging with the parents. It's important to foster a stance of enquiry and use the questioning approach. |
Suggested wording when contacting parents: |
|
"Hi, my name is …, I'm calling from the Department of Communities."
"My role is to investigate some worries that I've received in relation to your child, is it safe for you to talk at the moment?"
"We've received some worries about ....... abuse of your children and I'd like to organise a time when I can come to your home and talk to you more about this". |
|
3. Allow the parents the opportunity to respond The Department
must allow parents the opportunity to respond to the reported concerns and provide their account. It's critical that parents understand your role in undertaking an investigation that will require them to make a determination about harm. Whilst it may seem excessive to notify the parents of your role, failure to do so may mean that they are not fully informed of your statutory role in conducting an investigation and the seriousness of the situation, thereby denying them procedural fairness. Parents can respond to reported concerns by: - phone
- in person, e.g., at a home visit, or
- at a Signs of Safety meeting.
Suggested wording: |
|
"Thank you for letting us come over. As I said on the phone, my name is ……. and I work for the Department of Communities".
"My job is to complete a Child Safety Investigation and determine whether or not your child, (name), has or hasn't experienced harm".
"As part of that investigation I want to get your perspective on the worries that have been reported". |
|
4. Sight and/or interview the child You
must sight and/or interview the child during the course of a CSI. The Department places significant value on the voice of the child and this is one way to gather credible evidence.
Children who are at an increased risk of abuse, including neglect, should be prioritised for visits so that the child can be sighted regularly throughout the investigation. This includes High Risk Infants and children with disability and/or serious ongoing health issues. There are situations where you should insist on sighting a child, and this may include when the child is sleeping.
You should seek the consent of the parents to interview or sight the child as early as possible in the investigation. |
| A decision to delay sighting and/or interviewing the child or not to sight and/or interview the child
must be clearly documented and approved by your team leader. |
The Department
must have authority to interview a child, either from parental permission or under s.33 of the Act. You
must be an authorised officer with delegated authority under s.25 of the Act to use s.33. WA Police officers do not have authority under our Act to interview a child.
Detailed information about interviewing children is provided in the section 'Interviewing the child' below.
Suggested wording - requesting parental permission to interview a child: |
|
"Thanks for giving me so much information about your family. Part of our role is also to talk to children about what they think is going on for them."
"We think that what they have to say is really important. We usually talk to them at school because it's an independent place and somewhere safe for them."
"Would you be happy for us to arrange this? I would let you know when it was going to happen."
"I will contact you following the interview to either give you feedback over the phone or arrange to visit you again." |
|
5. Notify both parents of the likely outcome of the investigation You
must notify the parents of the likely outcome of the investigation before you complete your outcome report in the interest of procedural fairness. This allows the parents a final opportunity to express their views, ask any questions regarding processes and respond to the likely outcome. You can do this at: - a Signs of Safety meeting
- a home visit
- an office meeting
- by phone, or
- in writing if a face to face meeting or phone discussion is not possible.
Suggested wording: |
|
"Thank you for coming in to meet with us. As I've let you know before, my role was to conduct a Child Safety Investigation, which I've done and I wanted to talk to you about the likely outcome".
"As part of my investigation I've considered whether or not your child, (name), has experienced harm as a result of ……… abuse. My recommendation is that (name) has been harmed as a result of ……… abuse".
"This means that I will recommending that we substantiate …… harm and that the case remains open for Intensive Family Support so that the Department can continue to work with you to make sure that these worries are addressed".
"My decision has to be approved by my team leader. You can appeal my recommended decision by contacting my team leader and discussing the outcome directly". |
|
Procedural fairness / Natural justice Procedural fairness, also referred to as natural justice, is concerned with the procedures used by a decision-maker to obtain an outcome, rather than the actual outcome reached. Principles of procedural fairness should be applied to all decisions that may negatively affect the rights, interests or legitimate expectations of an individual, such as when identifying and recording a person assessed as Actual Harm Continuing Risk (AHCR). The following three principles underpin our processes:
The hearing rule – the decision maker must give an opportunity to an individual whose interests may be adversely affected by their decision the opportunity to be heard, before the decision is made.
The bias rule – the decision maker should be unbiased in the matter to be decided.
The no evidence rule – the decision that is made must be based on logical evidence (proven on the balance of probabilities – that is, there is a real possibility, that cannot be sensibly ignored, having regard to the nature and gravity of the feared harm in the particular case).
The Department follows the Western Australia Ombudsman's guidelines for procedural fairness - for details refer to their
website. All authorised officers should be familiar with the concept of procedural fairness and aim to promote this in their work.
Investigation by consultation (when we cannot have contact with the family)
You may undertake investigations, in exceptional circumstances, where you cannot or are not allowed to have direct contact with the family.
In these cases, it may be possible to gather sufficient information from other sources, such as the WA Police or an interstate child protection agency, to finalise the investigation.
An investigation by consultation requires that: the persons with whom the child protection worker is consulting must have direct contact with the child and the parents that each has had an opportunity to respond to the allegation (age and maturity permitting), and that each has had their responses considered.
You can then make a determination about whether or not harm is substantiated, and this completes the investigation by consultation. This method of investigation is recorded in Assist as "Investigation by Consultation".
Investigation not possible (when you have been unable to conduct an investigation)
There may also be exceptional circumstances when you are unable to conduct an investigation. You may have made multiple attempts to engage with the parents, locate the parents and/or locate the children with no success. You should discuss with your team leader if sufficient efforts have been made to conduct an investigation and whether the investigation outcome should be recorded as unable to investigate. If you make this decision you
must still complete an outcome report that details the efforts made to conduct the investigation and a plan for what should happen if the family comes to the attention of the Department in the future. Using Signs of SafetyYou must use the
Signs of Safety Child Protection Practice Framework when working with families and other agencies to develop cooperative relationships and better outcomes for children. Signs of Safety tools can be used throughout the investigation to promote the three core principles of: - Working relationships
- Munro's maxim: thinking critically, fostering a stance of enquiry, and
- Landing grand aspirations in everyday practice.
We must establish a working relationship with the child's parents and, if age appropriate, the child to resolve the issues that have led to the concerns. We should also take into account the networks of support that surround a child and seek to engage and include all stakeholders. For more information on Signs of Safety, including tools and resources, please refer to Chapter 2.2 Signs of Safety - Child Protection Practice Framework and the
Signs of Safety Hive. Harm statements, danger statements, and safety goals
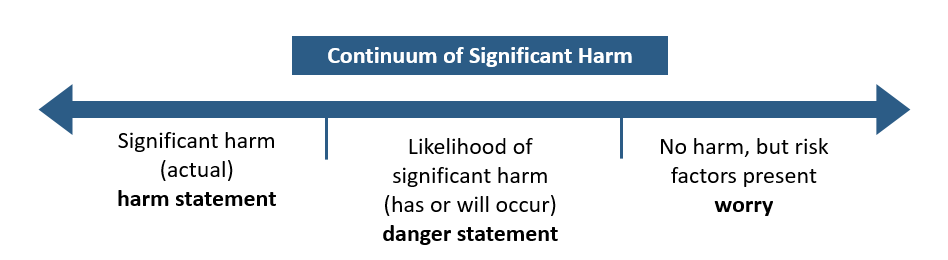
Harm statement: The description of who (name of person) caused harm to who (name of child) and the impact of that harm on the child. These are only created when the Department has already substantiated actual significant harm to a child.
Danger statement: The description of what the Department and others are worried might happen to the child in the care of their parents or carers in the future if the harmful adult behaviour doesn't change.
Safety goal:
Department safety goals - clearly describe the specific behaviours the parents or carers need to do for the Department to be confident that the child is safe.
Family safety goals - the family's ideas about what needs to happen to keep the child safe. The Department and family might agree to the same safety goal. You can use different tools to explain harm statements, danger statements and safety goals to children and families, for example: - Words and pictures
- Signs of Safety meetings
- The Three Houses
Intake and allocation
Internal Signs of Safety mappings: Many teams utilise internal Signs of Safety mappings at the point of intake or allocation to clarify the Department's grounds for involvement. Internal mappings utilising the three columns can be used by individuals or teams to clarify what we're worried about, what's working well and what we think needs to happen. It's critical that any harm statements, draft danger statements and safety goals are reviewed at this point. These must be developed if they have not yet been at this stage. Harm statements - articulate where harm has previously been substantiated by the Department. Danger statements - articulate the worries that relate to an abuse type under s.28 of the Act and articulate the possible subsequent harm. Each danger statement must only relate to one abuse type. Safety goals - identify the safety that we want to see for the child in relation to the harm and/or danger that has been identified.
For further information about harm statements, danger statements and safety goals, including how to develop them, please refer to the Signs of Safety Knowledge Hive. This is a great opportunity to review the complicating factors, which may include risk factors. It's critical to establish the missing information at this point and develop the plan/next steps that should be taken in the investigation. The scaling question should be used to determine how close/far away we are currently from the safety goal and the level of priority that needs to be given in actioning the next steps for the case. Meetings during the investigation
The three column mapping: The Signs of Safety framework encourages all practitioners to use the three column assessment and planning form when engaging with parents and families. The three column approach is designed to provide a balance between collaborative practice and professional, forensic assessment to generate a comprehensive, balanced child protection risk assessment. Three column mappings held with parents and family during an investigation should maintain a focus on the grounds for the Department's involvement (worries), what the parents/family are already doing to achieve safety (strengths) and a plan for addressing the remaining worries and generating sufficient safety for the children that the Department no longer has to be involved. You should utilise the Signs of Safety Assessment and Planning Form 255 to document any meetings and ensure that attendees are provided with copies on the same day wherever possible. For more information about Signs of Safety, including resources, refer to Chapter
2.2 Signs of Safety - Child Protection Framework. |
| It's not always possible to have a formal Signs of Safety meeting in an office with a whiteboard or smartboard available. The advantage of the Signs of Safety tools is that they are adaptable to your context. You can print a copy off and take it with you to meet with the family. |
Interviewing the childIf a child assessment interview was conducted as part of the Initial Inquiry, then a further child assessment interview (as part of the CSI) is not required. As part of a CSI, child assessment interviews should gather and clarify information, raise the topic of concern, give the child an opportunity to discuss any worries and initiate safety planning. A child assessment interview is not required if the child has made a disclosure of a criminal nature. In these circumstances the child must have a Specialist Investigative Interview only. This is to prevent a child being interviewed numerous times or any impact on evidence. In order to address the three practice requirements for a CSI, you must sight and/or interview the child.
|
| A decision to delay sighting and/or interviewing the child or not to sight and/or interview the child
must be documented and approved by your team leader. You must also document this decision in the CSI Outcome report.
|
|
| As far as practicable, the Department must support and fund the use of professional interpreters for any person who has difficulty understanding or communicating in English or whose disability prevents or restricts their understanding. This encourages the full participation of anyone who is not proficient in English and requires support to understand workers. For more information please refer to
Language and Interpreter Information and
Chapter 4.2: Language services - booking and payment.
|
For more information on CAIs, see Chapter 2.2 – Child Assessment Interviews.
Working with WA Police ForceIt is common that actions taken by the Department and WA Police Force intersect, especially when conducting CSIs that involve allegations of child abuse that meet the threshold for criminal investigation. You should liaise directly with WA Police Force when a criminal investigation coincides with a CSI and identify opportunities where actions can be undertaken jointly.
Specialist Investigative Interviews, previously known as forensic interviews, are conducted by trained interviewers from WA Police Force. Specialist Investigative Interviews are designed to capture victim or witness evidence relating to a criminal offence that will be admissible in a court of law. In the metropolitan area, these interviews are generally conducted by members of ChildFIRST and/or WA Police Force.
A Specialist Investigative Interview can only be conducted by a trained interviewer following determination that the case will require a joint response between the Department and WA Police Force during a Strategy meeting.
WA Police Force uses electronic equipement to visually record specialist interviews with children who: have made a clear disclosure that they have been sexually or physically abused have witnessed physical or sexual abuse of another child. or require other interviews at the discretion of WA Police Force.

| WA Police Force have trained interviewers in regional areas. Interviews conducted regionally are largely arranged locally with local detectives, however you can consult ChildFIRST at any time. |
Planning a joint response
All allegations of child sexual abuse reported to the local district office must be referred to and discussed with ChildFirst (metropolitan) or WA Police (regional) refer to entry 2.2. Sexual Abuse.
When you form a belief, on reasonable grounds, of the sexual abuse of a child you must refer to entry 2.2. Mandatory Reports of Child Sexual Abuse. All mandatory reports of child sexual abuse, once assessed, are sent by Mandatory Reporting Service, to WA Police.
When you become aware of a disclosure of physical abuse you must refer to WA Police using Form 523 Referral of Child Abuse to WA Police. ChildFIRST must be consulted if it becomes apparent that your investigation involves serious physical abuse or neglect likely to result in criminal charges being laid by WA Police. When WA Police receive a referral of alleged child abuse their duty officers assess whether WA Police have a potential role in conducting an investigation. You will receive one of the following responses: Where you receive an email specifying a single agency response you can continue with your investigative actions. If WA Police state they have a role in conducting an investigation then a joint strategy meeting should occur. The table below is a guide for how strategy meetings should be conducted depending on the context:
Sexual abuse
Metropolitan |
Regional |
Attendees: WA Police Force (detectives or Sergeant), Perth Children's Hospital Child Protection Unit, local district case manager and team leader, and others as appropriate.
Roles: Local district case manager and Team Leader will organise, chair and minute the meeting. An agreement will be reached about next steps relating to interview and any other investigative actions. Attendees: local WA Police Force, local district case manager and team leader, and others as appropriate e.g. local health service. |
Attendees: local WA Police Force, local district case manager team leader, and others as appropriate e.g. local health service.
Roles: Local district case manager to take the role of ensuring a strategy meeting is arranged and minutes taken. An agreement should be reached about next steps relating to interview and any other investigative actions.
|
Physical abuse
Metropolitan |
Regional |
Attendees: WA Police Force (detectives or Sergeant), Perth Children's Hospital Child Protection Unit, local district case manager and team leader, and others as appropriate.
Roles: Local district case manager and team leader will organise, chair and minute the meeting. An agreement will be reached about next steps relating to interview and any other investigative actions. Attendees: local WA Police force, local district case manager and team leader, and others as appropriate e.g. local health service. |
Attendees: local WA Police Force, local district case manager and team leader, and others as appropriate e.g. local health service.
Roles: Local district case manager and team leader to take the role of ensuring a strategy meeting is arrange and minutes taken. An agreement should be reached about next steps relating to interview and any other investigative actions. Recommend consult with ChildFIRST. |
Other There are exceptions to the above, and any time you are not sure about a joint response process you should contact WA Police Force to discuss further. Strategy meetings should all be recorded using
Form 850 Record of Strategy Meeting. WA Police investigations Any investigation by WA Police Force should not unnecessarily delay completion of a CSI. Actions such as safety planning and interviewing a person when it is proposed to record an Actual Harm Continuing Risk (AHCR) are critical to safeguarding children and should be completed in a timely manner. |
| The child's safety is the priority of
all investigations. |
It is important to be respectful and transparent while engaging with WA Police Force to promote ongoing working relationships and the best outcomes for the child involved.
Suggested wording: |
| "Hi, my name is ...... and I'm conducting an investigation into allegations that I believe you are also investigating. I wanted to introduce myself and see if there's any planning we could do together" "I'd be grateful for any information you could give me about the current police investigation and any next steps you plan on taking. This will help me in planning for my investigation." "Thanks for your email letting me know about your investigation. Some of the next steps I need to take include talking with the alleged perpetrator, which I plan to do on ....... date. Is there anything I should be aware of before proceeding with this?" "I need to conduct safety planning with the family to make sure that the children are safe, is there any way WA Police could be a part of that conversation?" "I know you might not be available to participate in safety planning with the family, what information are you comfortable with me disclosing to the family right now?" "I need to meet with the alleged perpetrator as we are planning on recording him as AHCR (provide an explanation) and the person is entitled to meet with us to discuss this. What information are you comfortable with me disclosing to the alleged perpetrator?" |
|
Assessing harmYou must make a determination at the conclusion of the CSI as to whether or not it is recommended that harm be substantiated. There are three outcome options: - Substantiated significant harm (actual)
- Substantiated likelihood of significant harm (has or will occur), or
- Not substantiated.
You should base any recommendation to substantiate harm on credible evidence gathered from a range of sources and relating to the abuse type that formed the grounds for their investigation.
| You should develop a harm statement whenever harm is substantiated. |
Actual significant harm |
Definition |
Based on a balance of probability, the child has suffered actual significant harm as a result of abuse or neglect. | |
Evidence |
There is credible evidence that the abusive/neglectful event occurred on one or more occasions and that the child has suffered actual significant harm which is demonstrated through their behaviour or other evidence. | |
Examples | 1. The child was physically abused when their parents hit them with a belt multiple times and there was actual physical harm as a result because they were left with bruises, welts and scars. 2. The child was sexually abused when their father sexually penetrated them and there was actual physical harm because they had internal injuries and emotional harm as a result because they said that they started self-harming as a result. 3. The child was emotionally abused when their father repeatedly hit, kicked and punched their mother and there was actual emotional harm as a result because they said they were terrified that their father was going to kill their mother and them and they have been displaying significant aggressive behaviours. |
Likelihood significant harm has occurred |
Definition |
Based on a balance of probability, the child is likely to have suffered significant harm as a result of abuse or neglect. | |
Evidence |
This decision must be informed by research on the known impacts of that type of abuse on the child and the credible evidence available to demonstrate how significant harm is likely to have occurred. | |
Examples | 1. Actual significant harm was substantiated for sibling 1, as a result of an incident of physical abuse, and the evidence is consistent that this incident of physical abuse occurred to sibling 2, but there is currently no evidence of harm to sibling 2. 2. You have assessed that the child has been sexually abused, but there is no evidence of impact on the child. 3. You know that a child has been present consistently during domestic violence incidents where the child's father has yelled at, hit and kicked the child's mother. You have no current evidence of impact on the child, but based upon substantial research and evidence you know it is highly likely that significant harm has happened to that child. |
Likelihood significant harm will occur |
Definition |
Based on a balance of probability, the child is likely to suffer significant harm as a result of abuse or neglect. | |
Evidence |
There is credible evidence of past/current harm and a likelihood that the harmful pattern of behaviour will continue and neither of the parents have the capacity to protect. | |
Examples | 1. The child's step-father was previously convicted of child sexual offences and the child's mother is non-believing and not protective, therefore it is likely that the child will suffer significant harm in the future as a result of sexual abuse. 2. You have substantiated physical harm of a sibling as a result of physical abuse by the father. You have identified significant ongoing risk factors which precipitated the previous physical abuse, including the father's drug and alcohol use and they are continuing.
3. You have been conducting pre-birth planning for an unborn infant who has two siblings already in care. You previously substantiated actual significant harm as a result of neglect when the siblings came into care, at the time the mother was using drugs and alcohol and failing to provide for their basic needs. The mother has continued to use drugs and alcohol and this is likely to significantly impact on her capacity to care for the newborn baby (neglect).
4. You know that the child's father has been physically and emotionally abusive to the child's mother, but you have not been able to gather any credible evidence that the child has been present during any incident, and there is no current evidence of impact (harm) to the child. The parents are continuing their relationship and deny that there is any potential impact on the child. You know from research and evidence about the impact on family and domestic violence on children that it is likely that significant harm will occur to the child as a result of emotional abuse - FDV if nothing changes. |
Assessment Assessment is the process of gathering relevant credible evidence in relation to the abuse type and harm you are investigating. Assessment is the ongoing process of receiving information, considering it in the context of your investigation and making a professional judgement about whether that information is credible. In your assessment, you should consider: - The types of evidence gathered and their credibility.
- The child's voice and the value placed on this.
- Patterns of behaviour, including events that led to the abuse and/or harm.
- Observations made of the parent's behaviour.
- Observations or information collected regarding the child's development and behaviour.
- Strengths that the parents and/or family have demonstrated and why this equates to safety.
- Missing information and the relevance of this in the investigation.
- Complicating factors and why they aren't worries.
- Barriers identified for the parents and/or family.
Refer to the
Child Development and Trauma Guide when articulating the impact on the child (harm). Analysis Analysis is making a determination about the abuse type and harm to the child, based upon the relationship between your assessment and the credible evidence of impact on the child. Your CSI is an analysis of the assessment information collected through the course of the investigation. The analysis should include reference to: - Severity - type and degree of harm.
- Vulnerability - age, development, functioning and opportunity.
- Probability - patterns, beliefs and complicating factors.
- Safety - strengths and protection.
The analysis should consider: Was the harm significant in nature and detrimental in effect on the child's wellbeing? What were the most important pieces of credible evidence that led to the conclusion regarding harm? If we are not substantiating harm, why? What evidence was lacking or what evidence was gathered that proved harm did not occur/will not occur? What actions/inactions have been observed of the parents? How does this relate to the harm of the child? How does this impact the child's safety and wellbeing? What has the child said or not said and how does this relate to harm of the child? What risk factors have been identified? How do these relate to the harm being investigated? Did the safety identified mitigate any substantiation of harm? If so, why? Has there been a time when the family were faced with a similar situation but were able to provide adequate care? What do we know about child development and how does this relate to our observations or information about this child? What do we already know about this family and harm? Is there a cumulative nature to the abuse this child has experienced?
Assessing a parent's capacity to protectYou must assess and analyse the parents capacity to protect their child. Section 28 of the Act refers to:
|
| You must assume that family and domestic violence is a factor in all cases and screen for this. As much as possible you should try to hold initial conversations with parents separately. This allows for FDV screening to occur, but also minimises the likelihood that the parents' will influence each others' recall of events.
|
|
| When you have identified parents involved in FDV you should consider their capacity separately. For example, the non-offending parent's capacity to protect their child is impacted upon by the perpetrator, as they are a victim of violence. You should think about any acts of resistance by the non offending parent to protect themselves or their children. |
Before continuing with the investigation, you should have: spoken to the parents separately and screened for FDV made observations about each parent's response to the concerns given each parent sufficient opportunity to respond to the concerns tried alternative approaches if you have been unable to engage with a parent consulted with others about ways to engage the parents, and reflected with colleagues who have also met the parents about their view of the parents' capacity.
Your investigation should take into consideration: Have the parents acknowledged the concerns? What is their current attitude to the concerns? What have the parents done to address the concerns so far? Have the parents demonstrated willingness to change? Do their actions reflect this? What have the parents done that shows they want to protect their child from further harm? Have the parents been open to the Department's suggestions? Have they been willing to engage with supports, services or counselling? Have they demonstrated change over any period of time? Are there barriers to the parents capacity to protect?
You need to make a determination regarding the parents: ability to provide a safe, stable and secure environment that will support the child's development; ability to regulate impulses and emotions; ability to empathise with and meet their child's needs; ability to identify and prioritise their child's needs ahead of their own; the parent's understanding of how their past behaviours (actions and inactions) are likely to cause harm to their child, and their capacity for, and willingness to change.
Frameworks for considering parenting capacity
Prochaska and Diclemente's "Stages of Change Model" The five stages of change: (adapted from
Child Neglect – Identification & Assessment by Jan Howarth) Pre-contemplation This is a stage where the parent is generally unaware that something is wrong. Parents tend to respond to professional concerns in a variety of ways: denying the problem, being angry towards professionals or being passive and helpless in their interactions. Contemplation The parent begins to recognise that there is a problem and that change may be necessary. At this point they weigh up the pros and cons of making changes. Determination At this stage the parent has decided to change their behaviour and looks into ways they might do this. Action This is the process of actively doing something. The parent chooses a strategy for change and pursues it, taking steps to put their decision into action. Maintenance This is a stage of conscious effort and attention to sustaining the strategies. Parents are more likely to succeed if the Child Protection Worker provides support and encouragement. Lapse or relapse This is where the parent either strays away from a strategy they have been using (lapse), or returns to previous levels and patterns of behaviour (relapse). This can happen if they are faced with an unexpected situation or crisis.
Indigenous Stages of Change |
| This is an example of another way to think about stages of change and the style of language that may make more sense for Aboriginal or Torres Strait Islander parents. When using this in practice the focus should be on how the person's actions e.g. drinking alcohol may affect their behaviour e.g. yelling at the kids. |
Not worried (pre-contemplation) Drinking has become a problem for the person in the centre of the circle. He or she is too close to drinking. The drinker isn't worried about his or her drinking. Family member (at the edge of the circle) is worried and wants the drinker to change but the drinker "can't listen". Thinking (contemplation) Something has happened to start the drinker thinking that there is a problem and that not everything about drinking is good. He or she has started to listen to what family is saying but still is not ready to change. Trying (determination) The drinker is halfway between grog and the family. The drinker wants to change and starts making plans to cut down or stop drinking. The person starts trying different things like light beer or not drinking on certain days. Doing (action) The drinker has made up his/her mind to change. He/she has now cut down or stopped drinking and has moved closer to family. It is still early days but changes have been made. Sticking to it (maintenance) The person no longer has a problem with drinking. He/she is sticking to the plan that was made. The problem drinking circle has been left and the person has moved back to family. Oops! Learning (relapse) The person has stopped drinking but has not learnt how to "say no" or hasn't found ways to be strong with other drinks. He/she may start drinking too much again. The person is learning new ways to stay strong. The family is helping the person. Copied from the
Cycle Of Behaviour Change, Living With Alcohol Program; Northern Territory Government 2000, Prochaska and DiClemente (1986). Toward a comprehensive model of change.
Addictive Behaviours: Process of Change, Miller and Heather, New York.
Domain of Parental Capacity
Capacity for change -
Basic care
-
Ensuring warmth
-
Stimulation
-
Guidance and boundaries
-
Stability
Resources for change -
The socio-economic environment
-
Their community
-
Their access to services
-
How the child, family and parenting functions within this
Willingness to change -
Desire or inclination
-
Readiness or eagerness
-
Preparedness
-
Cheerful compliance
-
Done voluntarily or ungrudgingly
Actual Harm Continuing Risk (AHCR) Criteria
For information on Actual Harm Continuing Risk, refer to the entry 2.2 Assessing a person as Actual Harm Continuing Risk (AHCR). Writing the Outcome ReportYou
must use the
Child Safety Investigation Outcome Report Template when completing the CSI outcome report. This ensures consistency across the Department and clarifies the expectations of you in completing the report. You can write the outcome report as soon as your investigative actions have gathered sufficient credible evidence to make a determination about:
Whether or not the child has experienced harm or is likely to experience harm as a result of the abuse
The parent's capacity to protect, and
Whether the child is in need of protection.
|
| It is up to you if you want to write the outcome report directly into Assist or into a Word document first and then copy into Assist. - Write short sentences and use dot points; use simple and clear language easily understood by everyone.
- Minimise the use of organisational jargon.
- All acronyms and abbreviations must be written in full when mentioned for the first time in your report. Include all the initials or abbreviations in brackets - for example, Chief Executive Officer (CEO), Department of Health (WA Health).
- All calendar dates should be written in text format - for example, 12 May 2015.
- Write in the 3rd person - for example, "Author assessed".
- Be mindful of the length of the report.
|
Template headings and information required
Family Group Who is the investigation related to? - Child (age)
- Parents
- Significant others
Grounds for investigation
What are we worried about? Summary of the information that was reported; incident; disclosure; date. For example: On 21 May 2018 the Department received a referral from Maylands Primary School that Sam (5 years) arrived at school upset and crying and disclosed to her teacher that 'last night' mum (Rebecca) 'punched me in my eye'. Sam was observed to have a round bruise to her left eye. Maylands Primary School advised that Sam has presented at school with previous bruising to her face in Term 1. The Department is worried that mum may have physically abused Sam and as a result a Child Safety Investigation was opened to assess harm or likelihood of harm.
Previous contact with the family. Summary of any prior investigation involvement relevant to this investigation; consideration around cumulative abuse and the impact of this or risk factors that may increase our worries; past harm; complicating factors. For example: The family have been known to the Department since 2015 for concerns pertaining to parental substance misuse (methamphetamine); mental health (diagnosed Depression) concerns for Rebecca; 8 contacts for Family and Domestic Violence (between 2015 – 2017) and Homelessness issues resulting in two Safety and Wellbeing Assessments for Sam (2015) for Neglect – outcome being not substantiated and (2017) Safety and Wellbeing Assessment for Emotional Harm- Family and Domestic Violence with the outcome being Substantiated Likelihood of Harm. Rebecca is known to the Department as a child in the care of the CEO from 1998 – 2007 for substantiated Neglect. Bill is known to the Department as a perpetrator of Domestic Violence towards Rebecca (2015 – 2017) as well as two previous relationships (2010 and 2012).
Initial assessment/draft danger statements (commencement of your analysis). What is the initial assessment (judgement) of the information whereby the case requires further action under an investigation. Summarise our concerns; link this to abuse type/possible harm/likelihood of harm to the child if further investigation is not undertaken. Include strengths, safety, complicating factors, missing information and draft danger statements. For example: The Department is worried that Rebecca punched Sam in the eye leaving her with a bruise and crying and upset. If Rebecca physically abuses Sam this could lead to Sam having bruises, broken bones or being seriously injured (physical harm), Sam could also feel scared, upset and like her mum doesn't love her (emotional and psychological harm).
Next steps to progress CSI. Summary of recommended next steps to gather credible evidence to formulate assessment and analysis of harm to the child; consider any missing information. For example: Does this include interviewing the child or just sighting the child within the environment? Does this include referral to police? Has there been FDV screening or does this need to be completed? Does this include any section 23's to gather further information? Does this include contact with the police to obtain criminal history / background / knowledge of family or address etc Does this include making contact with the school / other support networks?
Scaling question (initial judgement). On a scale of 0 to 10, with 0 being we are extremely worried for the child's safety and the child is in need of protection and 10 being that there are no worries and the case can be closed, where do you scale?
Action taken
What did we gather in terms of credible evidence? Summary of the critical events or actions and credible evidence that was gathered to inform this outcome. This is not a chronology of all the activities taken. -
Do not - copy and paste.
-
Do - summarise interviews and outcome of each action taken that is listed.
For example: Three unannounced home visits to sight the home environment
(Objective reference QA111111) Specialist child interview (SCI) for Sam in which Sam made a consistent disclosure (Objective reference QA111112) Medical assessment of Sam pertaining to her bruise (Objective reference QA111113) Two Signs of Safety meetings
(Objective reference QA111114, QA111115) Liaison with school to gather evidence around Sam's presentation and wellbeing
(Objective reference QA111116, QA111117) Liaison with Police (WAPOL) inclusive of obtaining criminal history
(Objective reference QA111118) Safety planning meeting with the safety network (Objective reference QA111119, QA111120). Decision not to sight and/or interview the child with Team Leader approval (Objective reference QA111367)
Harm analysis and parents' capacity to protect Analysis is making a determination about the abuse type and harm to the child, based upon the relationship between your assessment and the credible evidence of impact on the child. Your CSI is an analysis of the assessment information collected through the course of the investigation. Your analysis should include reference to:
Severity - type and degree of harm.
Vulnerability - age, development, functioning and opportunity.
Probability - patterns, beliefs and complicating factors.
Safety - strengths and protection.
Your analysis should consider: Was the harm significant in nature and detrimental in effect on the child's wellbeing? What were the most important pieces of credible evidence that led to your conclusion regarding harm? If you are not substantiating harm, why? What evidence was lacking or what evidence did you gather that proved harm did not occur/will not occur? What actions/inactions have you observed of the parents? How does this relate to the harm of the child? How does this impact the child's safety and wellbeing? What has the child said or not said and how does this relate to harm of the child? What risk factors have you identified? How do these relate to the harm you are investigating? Did the strengths you identified equate to safety? If so, why? Has there been a time when the family were faced with a similar situation but were able to provide adequate care? What do you know about child development and how does this relate to your observations or information about this child? What do we already know about this family and harm? Is there a cumulative nature to the abuse this child has experienced?
Parent's capacity to protect |
| Do not consider this section when a child is in the CEO's care. This is an opportunity to examine the care arrangement. |
You
must make a determination about both parents' capacity to protect their child in the context of the abuse type and harm you have assessed. Here you must define: Do the parents have capacity to protect? Yes/No What is your evidence for your determination? Please refer to the section
'Assessing a parents' capacity to protect' above for guidance about what you should include in your assessment.
Key decisions and rationale These are statements and should be clear and concise. Is the child in need of protection? Record the AHCR criteria (if it has been applied). Document your final harm statements (where actual significant harm is being substantiated), danger statements (where likelihood of significant harm is being substantiated) and safety goals. Include a decision statement of: Has the child suffered actual significant harm. Is there a likelihood of significant harm - on a balance of probabilities it is more likely than not that the child has or will suffer significant harm. Whether you are recording someone as AHCR or placing an alert on the system in relation to a person. Whether the parents have protected the child from harm or are they likely or able to protect the child from harm or further harm. Are further actions required to safeguard the child, such as Intensive Family Support or Intervention Action. Is safety planning required?
|
| If you are completing the CSI outside the 30 calendar day timeframe, include a rationale for in the key decisions and rationale section. |
AHCR criteria
This can only be considered when actual significant harm has been substantiated. Please refer to the Actual Harm Continuing Risk (AHCR) criteria page for complete information about when consideration of this criteria is required and how to apply the criteria.
Plan Actions from the CSI can include the following: No further action. The provision of social services
s.21(1)(a). The provision of Intensive Family Support Services
s.32(1)(a). Arranging or facilitating a meeting between key stakeholders to develop a plan to address the ongoing needs of the child
s.32(1)(b). Entering into a negotiated placement agreement s.32(1)(c). Take, or cause to be taken, intervention action in respect of the child
s.32(1)(e). Take, or cause to be taken, any other action in respect of the child that the Department considers reasonably necessary
s.32(1)(f). Further actions by the CEO before a child is born
s.33B(a)(b)(c).
The following actions can be taken if the child protection worker forms a view that the child may be in need of protection: take a child into provisional protection and care with a warrant
(s.35 and s.123). take a child into provisional protection and care without a warrant
(s.37 and s.38). make an application for a protection order
s.44. provide a service response to the child and family if required, whether or not the child is in need of protection
(s.32).
Other considerations: What do you want to happen if this family come to the Department's attention again? If you have recorded someone as AHCR, make note of that here and that it will require review at next contact.
Assist recording options (grounds for CSI) |
| Be aware! When you enter this information in Assist there may be more options available to you. The status and outcome options detailed below are the recording options that you must follow. |
Record the following types of abuse according to guidance in the table below:
Abandonment -
s.28(2)(a)(i)(ii)
Dead or Incapacitated -
s.28(2)(b)
|
|
You
must not record substantiated or not substantiated as a status or outcome. This section of the Act
does not allow for an investigation and determination about harm. |
Status and outcome recording options |
What does this recording mean? | Status choice: - No suitable adult OR suitable adult
Outcome choice: - No suitable adult OR suitable adult
| The status and outcome of the CSI are a record that you either were able to locate the child's parents or a suitable adult relative or other suitable adult who was willing and able to care for the child or not. If you were unable to locate the parents or another suitable adult (no suitable adult), then you would be progressing to intervention action. |
Record the following types of abuse according to guidance in the table below:
Physical Abuse -
s.28(2)(c)(i)
Sexual Abuse -
s.28(2)(c)(ii)
Emotional Abuse -
s.28(2)(c)(iii)
Neglect -
s.28(2)(c)(v)
Unable or unwilling to provide adequate care -
s.28(2)(d)(i) & (ii)
Status and outcome recording options |
What does this recording mean? | Status choice: Outcome choice: |
Status: Did not investigate - you made a decision not to investigate this. Unable to investigate - despite your best efforts, you were unable to take any investigative actions to assess the reported abuse and any subsequent harm. Not substantiated - there is insufficient evidence to suggest that the child has or will suffer harm as a result of the abuse/neglect. Substantiated Harm - there is sufficient evidence to substantiate that actual harm occurred to the child as a result of the abuse/neglect. Substantiated Likelihood Harm - there is sufficient evidence to substantiate that it is likely that the child either was or will be harmed as a result of the abuse/neglect.
Outcome: Discontinued - the investigation into this abuse type is being discontinued as it was not required. Not substantiated - as above. Substantiated Harm - as above. Substantiated Likelihood Harm - as above. Unable to complete investigation - you made attempts to undertake the investigation, despite this you were unable to gather sufficient evidence to make any determination about whether or not harm occurred. |
ApprovalsThere are different lines of approval depending on the circumstances relating to a CSI, they are listed below. Someone who is able to review and approve Child Safety Investigations is now referred to as a CSI Reviewer. All CSIs
must be quality assured in order to be approved. CSIs will be quality assured by CSI Reviewers. CSI Reviewers
must be Level 6 or above.
A CSI Reviewer cannot endorse or approve a CSI they have written themselves.
When there is no recording of AHCR and the CSI does not relate to a child in care of the CEO the team leader can approve the outcome, provided they are a CSI Reviewer.
For information about the formal review process of a completed CSI, including AHCR reviews, please refer to the entry 2.2 Child Safety Investigation Review Process. CSI Reviewers
What is a CSI Reviewer?
A title given to anyone, Level 6 or above, who has participated in the CSI Reviewer training.
All team leaders will be required to complete the training to become a CSI Reviewer and be able to quality assure and approve CSIs.
What does a CSI Reviewer do?
Quality assure the content and actions within a CSI.
Provide feedback to CSI authors.
Approve CSIs when appropriate (depending on the nature of the investigation - see tables below).
Review completed CSIs when a request has been made for the investigation and/or outcome to be reviewed.
Approval delegations |
If…
|
Then…
| You recommend the outcome be recorded as discontinued or unable to complete investigation (pre-birth to under 3 years)
| Team Leader endorsement and District Director approval
| |
You recommend the outcome be recorded as discontinued or unable to complete investigation (aged over 3 years)
| Team Leader approval
| |
You recommend harm is
not substantiated
| Team Leader approval
| |
You recommend likelihood of harm is substantiated
| Team Leader approval
| You recommend actual harm is substantiated and you have determined no-one will be named as AHCR - no AHCR is recorded
| Team Leader approval
| You recommend that actual harm is substantiated, and you have determined someone will be named as AHCR - AHCR is recorded
| Team Leader endorsement and District Director approval
| Naming a child under 18 years of age as AHCR | Team Leader endorsement and District Director approval, following consultation with General Manager, Specialist Child Protection Unit
| Local district director and the General Manager, Professional Practice Unit do not agree on the naming of a child under 18 years of age as AHCR | District Director has final decision and approval | Review of person's AHCR status at subsequent contact, such as CSI (not a CSI Review), results in a recommendation to change the person's AHCR status | Team Leader endorsement and District Director approval | CSI Review | District Director approval | | Contentious CSI Review completed outside the district | District Director with Executive Director Service Delivery endorsement |
CSI Approval delegations specific to Children in Care (approved carers, Community Service Organisations and employees).
If…
|
Then…
| | You recommend harm is not substantiated | Team Leader endorsement and District director approval
| You recommend likelihood of harm is substantiated
| Assistant District Director endorsement and District Director approval
| You recommend that actual harm is substantiated, and you have determined no-one will be named as AHCR – no AHCR is recorded
| Assistant District Director endorsement and District Director approval
| You recommend that actual harm is substantiated, and you have determined the carer will be named as AHCR – AHCR is recorded
| District Director endorsement and relevant Executive Director approval
|
Actions following approvalYou
must select a next action when completing a CSI. The actions available for selection depend on the outcome recorded in relation to harm, but they may include: The provision of social services
s.21(1)(a). The provision of Intensive Family Support Services s.32(1)(a). Arranging or facilitating a meeting between key stakeholders to develop a plan to address the ongoing needs of the child
s.32(1)(b). Entering into a negotiated placement agreement
s.32(1)(c). Take, or cause to be taken, intervention action in respect of the child
s.32(1)(e). Take, or cause to be taken, any other action in respect of the child that the Department considers reasonably necessary
s.32(1)(f).
|
|
If you are completing a CSI for a child in the CEO's care you cannot take intervention action. You
must choose either 'no further action' or the 'the provision of social services'. |
Assist will require you to select a next action to proceed. Your selection should correlate directly to the determination and recommendation made in your CSI outcome report. For specific procedures relating to the different options please refer to the entries below: Notifying parents and/or other significant people You
must notify the parents and/or other significant people of the outcome of the CSI. This should include notifying the child, in an age appropriate way. The notification should be done in writing where possible using the CSI Outcome letter (Forms 230,
231 or
233 in related resources) and a copy of the letter placed on the client file..
|
| It may not always be possible or appropriate to notify people in writing of the outcome of the CSI, for example, they may have no fixed address or be unable to read. You
must still make every effort to communicate the outcome verbally and place a case note of the discussion on the client file.
|
The information in the outcome letter should not come as a surprise to the person receiving it, especially if harm has been substantiated. If you have followed the investigative actions listed here then the significant people should have already been notified of the likely outcome of the investigation and given the opportunity to respond to this. |
| Significant personalisation of the outcome letter is not recommended. It might be appropriate to include phrases like: "Thank you for working with us during the time" or "We have appreciated your cooperation during this investigation and wish you and your family all the best in the future". You should be wary of over-personalising the letter and making unnecessary inclusions that might not be endorsed by the Department. |
|
If… |
Then… | The outcome letter is for a CSI where harm was not substantiated | A team leader can sign it | | The outcome letter is for a CSI where likelihood or actual harm was substantiated and there is no established AHCR | A team leader can sign it | | The outcome letter is for a CSI where actual harm was substantiated and there is established AHCR | A district director
must sign it | | The outcome letter is for a CSI where the child is in the CEO's care and likelihood or actual harm was substantiated and there is no established AHCR | A team leader or assistant district director
must sign it | | The outcome letter is for a CSI where the harm occurred before a child entered the CEO's care and likelihood or actual harm was substantiated and there is no established AHCR | An assistant district director
must sign it |
|
|

